I've had a pound of chicken livers from the farmers market locked away in the freezer for quite some time. The girlfriend isn't exactly dying to eat them, so I needed to wait until she was out of town. But I still had to figure out what to do with them. Fortunately, one of my colleagues is a former chef, and when I told him about my stash of offal, he eagerly offered me a recipe. Chicken liver mousse makes the medicine go down smooth.
Liver is the original multi-vitamin. I'm generally cautious about parsing foods based on their vitamin, mineral, or other micronutrient content. After all, it's hard to be nutrient deficient, or insufficient, when your main foods are vegetables, meat, and dairy. So looking at nutrient content is almost a moot point. But liver is worth talking about.
Either cherished or despised, this vital organ provides compounds that are hard to squeeze out of standard muscle meat, such as choline and vitamin A, and provides more B vitamins than anything else.
The graphs below show the vitamin content of 3.5 ounces of chicken liver, 1.75 ounces of chicken liver (an amount that could reasonably be eaten in a night's worth of pâté), and 3.5 ounces of chicken breast tenders, all cooked. Vitamins are measured in different units, such as international units, milligrams, or micrograms, so it's only valid to compare the vitamin contents between the foods, and not between the different vitamins. Two graphs are shown since some vitamins simply come in higher numbers (vitamin A) than others (choline), and I didn't want to do any crazy graph standardizing on Christmas Day. A quick glance shows that the amount of choline and vitamins A and B12 in liver compared to breast meat is remarkable. Whether you're an obligate carnivore, or mostly vegetarian, the occasional liver dish would be a nice way to round out a diet.
Fig. 1 Vitamins with smaller numbers
Fig 2. Vitamins with larger numbers
But enough with the lecture. The mousse is rich, slightly sweat from the Madiera, and a way to use up the somewhat obscure chicken livers that might otherwise be discarded before roasting a whole bird. There isn't a lot of liver taste, I promise. But I still have to see if the girlfriend approves. Merry Christmas!
Chicken Liver Mousse
Here's what you need. And yes, it's essentially a 1:1 ratio of butter to liver, by weight.
Ingredients: 1/2 pound chicken livers, 1/2 pound butter, Madiera, water, salt and pepper.
1. Poach the chicken livers in a 50:50 mix of Madiera and water, or 1 cup of each, over medium-high heat. Cook for no more than 3 minutes. You want the livers cooked to rare or medium-rare, as overcooking them will negatively affect the puree.
2. Set the livers aside. Reduce the cooking liquid to just under 1/4 cup. In the mean time, cut cold butter into 3/4 inch cubes.
3. As the cooking liquid approaches the right volume, puree the livers in a food processor using small pulses. Then, turn the processor ON, and add butter, one cube at a time. Hit it with a few splashes of fresh Madiera as you go.
4. Add the reduced cooking liquid (it should be a rich brown color) to the processor. Salt and pepper to taste. Process to incorporate.
5. Spread the mousse into a shallow ramekin. Cover tightly as you would guacamole, and remember that all of the iron in the liver will oxidize and brown when exposed to air, so make sure you keep it covered when it is stored. Let it set-up in fridge for one hour. The dish can easily be made the morning or night before, and stored in the fridge.
Serve over toasted baguette with thinly sliced blanched asparagus, along with a nice glass of Pinot Noir.
In many ways, medicine is remarkably similar to farming. The ancient Romans and Chinese, for example, knew that rotating crops and spreading manure in their fields would vastly improve yields. These farmers didn’t know the underlying biology, and it didn’t matter: these practices worked, and they worked well. Often, medicine is little different. Insulin was given before knowing that it spurred the movement of glucose transporters to the edge of muscle cells, and exactly how acetaminophen relieves headaches has remained elusive. The bacteria that thrive in yogurt and kefir, otherwise known as probiotics, are the modern day equivalent of manure. But researchers are beginning to get a grasp of the microbial world in our tummies.
In a paper published last month, Jeffrey Gordon’s team at Washington University in St. Louis identified how probiotics may influence gut health. The scientists inoculated a sterile mouse model with 15 strains of bacteria that normally reside within the human colon. The mice were then given probiotics and studied for changes in gut function.
Source: Wikipedia. The model bacteria e. coli viewed by electron microscopy
The most interesting finding was that the probiotics hardly changed the composition of the bugs in the gut. That is, the beneficial bacteria didn’t simply displace the ones already residing in the animals’ intestines. And this makes sense to Gordon, who when interviewed said that the bacterial-colonization idea was analogous to “pouring a gallon of Kool-Aid into your swimming pool and expecting it to turn red.”
Instead, the new bacteria apparently vary the gene expression of the native ones.
Human cells and all of the microbes that inhabit the body have individual sets of genes. A combination of spontaneity, interactions with other genes, and environmental triggers causes the genome to produce chains of messenger ribonucleic acid (mRNA). The “expressed” mRNA, in turn, is converted, or “translated,” into chains of amino acids (proteins) that do all the wonderful things that cells – or bacteria – do. If genes were sheet music, the mRNA would be the specific keys, or group of keys, that produce the distinct musical notes or chords. Probiotics changed the frequency that the bacteria’s genes produced mRNA, like a pianist using fewer C’s and more major scales. Different levels of gene expression, like different musical composition, produce different effects.
Source: Wikipedia. Gene coding a protein.
The most noticeable shift in expression was seen in genes that dictate carbohydrate metabolism, specifically molecules known as xylooligosaccharides that are commonly found in plants. Importantly, the probiotics manipulated the same genes in the bacterial community of human subjects. It’s these sudden manipulations that may explain the known benefits of friendly microbes.
Gut bacteria influence the entire body. Clinical trials have consistently shown improved gut function in people taking probiotics, where the benefits are especially pronounced in those afflicted with diarrhea. When mice are fed probiotics, the brain produces chemical critical for regulating anxiety. Conversely, eliminating native bacteria can be detrimental. Some scientists are considering the over-use of antibiotics as a contributor to the rising incidence of allergies, asthma, and inflammatory bowel disease because the drugs indiscriminately wipe out the pathogenic and helpful bugs. And eating bacteria isn’t the only way to get them into the gut.
Fecal transplant is the most remarkable bacterial therapy, if not the grossest. As the name makes obvious, the treatment takes feces and the billions of resident bacteria from one person and transplants it into someone else. It has been used in several different conditions, but the most dramatic results have been shown in c. difficile infections, a relentless hospital acquired bug that is rapidly resisting more antibiotics. The stomach-churning therapy resolves a whopping 9 out of 10 c. difficile cases with virtually no side effects, and apparently, no smell. What this frontier of probiotics will evolve into, though, is still an open question.
Both scientists and marketers are pushing the frontier of probiotics. “Contains live active cultures” is plastered on every dairy product from yogurt to ranch dressing. Unfortunately, promise before understanding is a simple recipe for bad nutrition. Bacteria could become the new snake oil, like high-dose antioxidant supplements. But microbiologist Jeffrey Gordon’s experiments offer a model to begin rigorously investigating how probiotics work, optimal combinations of bacterial strains, and appropriate doses.
The great 20th century physicist Richard Feynman once said that “what I cannot create, I do understand.” It looks like the science of probiotics is taking a step in the right direction.
What if you could take a pill that would simply melt your fat away?The dream has become reality, but you have to be a chubby monkey to get your hands on it.
Barnhart and colleagues performed a placebo-controlled trial on adipotide, an experimental new drug to combat obesity, in obese rhesus monkeys.Adipotide acts to slowly destroy the blood vessels that feed fat tissue.By starving fat cells nutrients and oxygen, the cells eventually die, and fat loss ensues.The compound has shown considerable success in rodents, but in order for the drug to progress into human trials, the experiments had to be replicated in non-human primates.Indeed, the results are promising.
Spontaneously obese monkeys were given daily injections of adipotide, or placebo, for 28 days, followed by a 28 day recovery period.The treatment group enjoyed a 15% weight loss, on average, by the end of the eight weeks – equivalent to a 275 pound person losing 40 pounds.The bulk of the fat loss was visceral fat, which is the most deleterious region to carry body fat.
There is still plenty of time until it could be use to treat human obesity, but until then, the drug’s actions on fat tissue are interesting to ponder.
Souce: Wikipedia. Adipose (fat) tissue.
The yellow fat cells are usually supplied by the red blood vessels.
Adipotide is a protein-based compound that binds to the endothelial cells that line the vasculature of fat tissue.The protein enters the cells and causes them to commit planned suicide, or “apoptosis” in biology-speak.Deprived of blood, the fat cells progressively die-off as they starve of oxygen and nutrients.The fatty acids and triglycerides within the cells are released into the circulation and the body cleans-up the debris, leaving the monkeys svelte.But where does the fat go?
One would expect a flood of triglycerides into the blood stream.This is called hypertriglyceridemia and is a component of the metabolic syndrome and is a risk factor for heart disease.However, this doesn’t appear to be the case.The animals’ blood lipids improved throughout their weight loss.What’s more, the animals became considerably more insulin sensitive – an important improvement that prevents diabetes and other complications of obesity.Together, these data suggest that the freed fat was successfully oxidized, or “burned”, by the body for energy.
Throughout the treatment period, the monkeys receiving adipotide consumed fewer “biscuits” than their overweight controls.The authors attribute the poor appetite to enhanced satiety, rather than nausea, which in turn led to weight loss.
However, adipotide did not cause lean monkeys to eat less.The selective effect on appetite suggests that eating less isn’t the primary effect.And after all, the drug targets the fat cells, not the brain.Rather, it seems plausible that the dying fat cells free up an abundance of fat to be used for fuel.With plenty of fuel available to the body, there’s little reason to stock up on biscuits.
There isn’t any data measuring the type of fuel – carbohydrate or fat – metabolized by the monkeys, so the mechanism requires a bit of speculation.
The monkeys lose fat mass into the circulation, which gets oxidized for energy.Fat loss improves insulin sensitivity, so the animals don’t have to secrete as much insulin in order to compensate for insulin resistance.Plenty of fat for energy in the presence of lower insulin – remember, insulin drives fat storage – allows the monkeys to get by with eating less.It’s like a drug-induced low carb diet, but instead of a bun-less cheeseburger, the monkeys are able to dine on their fat stores.Although the cheeseburger would have one less side effect.
Source: Wikipedia. A lean (and wild) rhesus macaque
The experimental monkeys showed transient problems with their kidneys, as indicated by elevated creatnine levels and slight microscopic damage to the tissue.It’s unclear from this study whether the problem stems from the drug itself or a complication from the dying fat cells.Side effects are especially problematic if adipotide needs to be taken chronically.
The monkeys started to show some regain of weight by the end of the four week recovery period, but the amount was minimal.This could be an inherent problem to the drug, or it could be because they stuck to their low-fat junk food diet - monkey chow composed of 59% carbohydrate, 28% protein, and 12% fat – that made them fat in the first place.
Over lunch today (chicken along with butternut squash topped with butter and cinnamon, in case you were wondering), I came across a couple of links that really hit the mark. The first is a LA Times article on the current science of antioxidants.
Source: Wikipedia. Oxidized iron, or better known as rust.
Everyone wants to avoid oxidation, whether it's the browning of apples or one of the mechanisms behind aging. The latter phenomenon is why everyone hunts down antioxidant rich foods. Fortunately, it seems that every food has some sort of antioxidant (even butter has vitamin A!), but some foods are particularly high in certain antioxidants (think pomegranates). So, the theory goes, oxidation is bad, foods have antioxidants, so let's eat a whole lot of selects foods - or squeeze the antioxidants out of them - to ward of oxidation and subsequent aging and disease. Or maybe it's not so simple.
This article basically sums up my entire opinion of antioxidants. Yes, we probably need antioxidants. But we don't know nearly enough about biological oxidation and dietary antioxidants to be able to come up with a miracle diet or formula to prevent disease. And it appears that our body even uses some oxidation to its advantage, as a previous study has shown that high doses of antioxidants can prevent the insulin sensitizing effect of exercise. So my rule of thumb for antioxidants, avoid the foods that don't have them, which just so happen to be white flour, white rice, and sugar. How convenient.
And if you have fifteen minutes, here is an excellent talk by a physician turned epidemiologist. He discusses the major problems of epidemiology and newspaper headlines, and the serious ethical dilemmas we are encountering with large pharmaceutical trials. He also mentions the publication bias problem that I mentioned in my meta-analysis post.
Source: Wikipedia. I would have had some if it looked this good...
There’s few things more ironic than walking into a lecture titled “the molecular biology of hepatic steatosis” and being met by a table stacked with pizza and soda.Of course, the molecular biologists in the crowd weren’t the ones with non-alcoholic fatty-liver disease (or NAFLD), but it’s hard to ignore the dissonance.Fortunately, the talk was better than the lunch offerings.
The lecture was by a medical researcher who investigates the molecular mechanisms behind fatty liver disease.Today he was highlighting his group’s most recent work on the molecular mechanisms connecting obesity to liver fat deposition.
Source: Wikipedia. Adipocytes (fat cells).
The researcher wanted to address several hypotheses.The first hypothesis is that when people become obese, their fat cells enlarge (rather than multiply) to a point that induces cellular stress.This stress then produces a cascade of intracellular signals that tell the fat cell (adipocyte) to begin apoptosis (intentional cell death).The troubled fat tissue then secretes deleterious cytokines, or hormone-like chemicals.
Source: Wikipedia. A Macrophage.
The second hypothesis is that these cytokines recruit immune cells – specifically macrophages, an important cell of the innate immune system – that begin to engulf the fat cells.The combination of dying fat cells and macrophages causes a big problem.
When fat cells become too large, and start dying off, they dump their fat content into the circulation – like an overstuffed cream-filled donut.This results in a surplus of free fatty acids floating around the body.And this is important because two-thirds of the fat in the livers of people with NAFLD are derived from the circulation.And it isn’t just the adipocytes causing trouble.
Macrophages enjoy company, so they recruit more macrophages by secreting cytokines that have wonderful names such as Tumor Necrosis Factor alpha and Interleukin-6.These chemicals, and many others, create a vicious cycle whereby inflammation produces more inflammation produces more information.The inflammation in the fat then appears to spill out into the circulation and reach the liver.
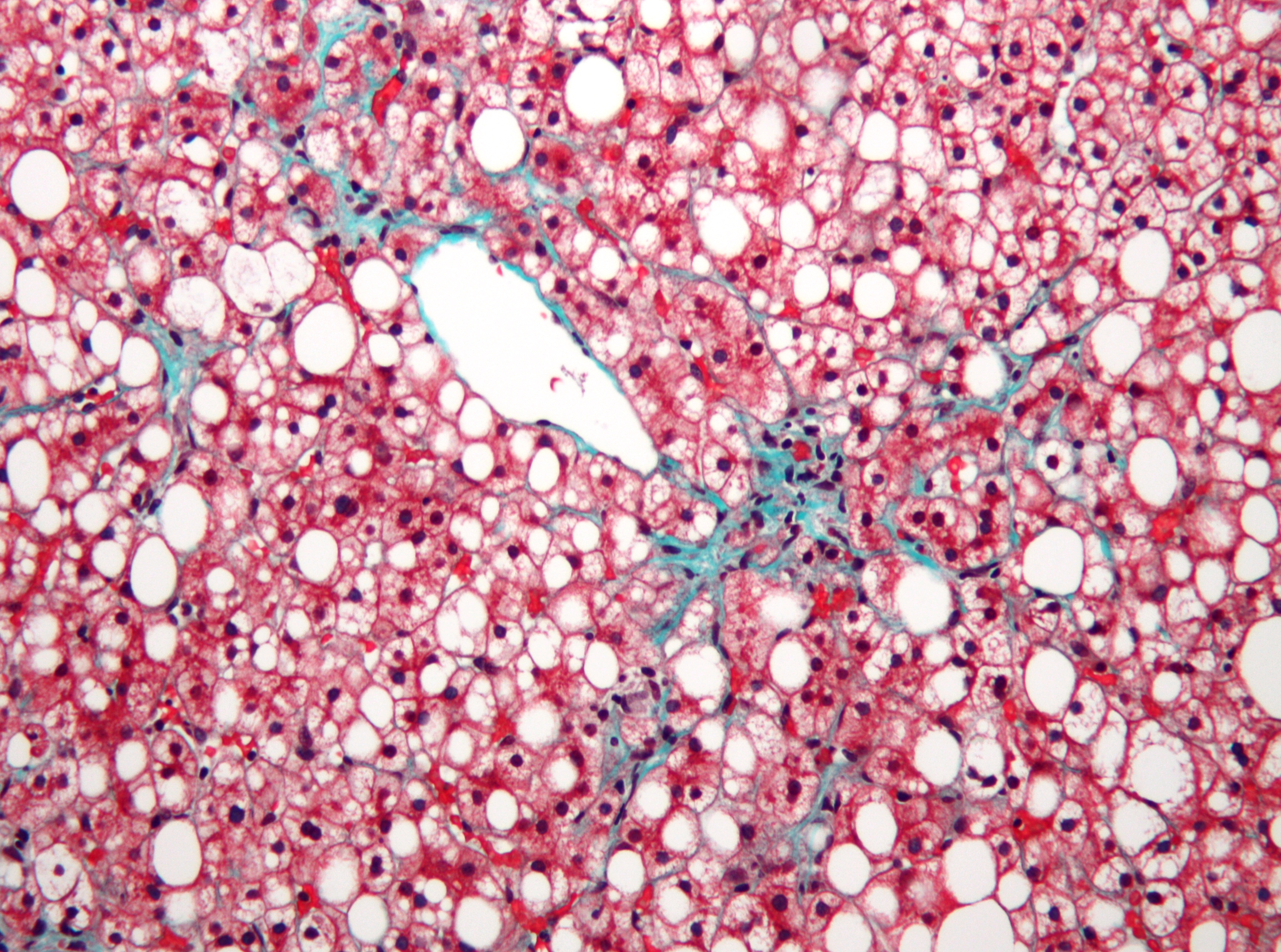
Source: Wikipedia. Not-alcoholic fatty liver disease.
Liver cells are pink, the white is fat that shouldn't be there...
Inflammation in the liver leads to dysfunctional fat metabolism.The liver then begins producing too much fat, which also accumulates in the liver.The excessive free fatty acids in the circulation and the dysfunctional fat metabolism in the liver account for virtually all of the excess fat seen in NAFLD.This fat then begets more inflammation.
The excessive fat and inflammation in the liver, and the fat from inflammation, generate a lot of oxidative stress in the liver.This oxidative stress produces more inflammation, and causes the liver cells to dye off.This can lead to a clinically inflamed liver (steatosis hepatitis) and even cirrhosis (think alcoholic). At least, according to the researcher's hypothesis.
The researcher had plenty of data from cell cultures and mice, each experiment clearly showing an increase in relevant proteins and genes in response to diet-induced NAFLD.He also cited a clinical trial that showed that vitamin E (an anti-oxidant) supplementation was more beneficial than the insulin-sensitizing drug metformin in patients with confirmed NAFLD.Although, admittedly, the anti-oxidant treatment didn’t seem to be that much of a better treatment.But perhaps oxidation is indeed the culprit, and Vitamin E just isn’t a strong enough anti-oxidant.
The obesity to inflammation to fatty liver (and other problems) is a compelling hypothesis, and it has plenty of support in the research community.If this hypothesis with stands the test of time, then it would support the notion that whatever makes us fat (sugar ‘cough’ and ‘cough’ white flour), probably also leads to insulin resistance, fatty liver, and all the other diseases associated with the Western diet.But however it goes, I’m still glad that I brought tuna, broccoli, and buttered brown rice instead of chowing down on cheap pizza and soda.
"If one is going to make recommendations about how to optimize one's diet, one has to consider what kind of calories are going to take the place of those from saturated fat." - Ronald Krauss, M.D.
While few may characterize his research in such a way, Ronald Krauss has been investigating the law of unintended consequences as it applies to nutrition. Krauss has demonstrated, in obese people and people with impaired metabolism, that replacing dietary saturated fat with carbohydrate, especially refined carbohydrate, will not improve the overall blood-lipid profile, and will actually make it worse. Reducing one nutrient requires careful consideration of what it will be replaced with.
Denmark has introduced a tax on foods that are high in saturated fat. The tax will be applied to foods that contain 2.3% saturated fat, although it is unclear whether this means 2.3% of calories or by weight. Presumably, this tax is intended to reduce the production and consumption of foods that ostensibly lead to cardiovascular disease (CVD). But there are a few problems with this.
As I've written on my blog, the reduction of dietary saturated fat does not necessarily lead to reduced risk of cardiovascular disease. If you decrease a macronutrient, you must consume something in its place. Replacing saturated fat with polyunsaturated fat reduces the risk of CVD, but does not lower the risk of CVD mortality or total mortality. It is not certain whether replacing saturated fat with monounsaturated fat or unrefined carbohydrates will reduce CVD risk. And replacing saturated fat with refined carbohydrates - white flour and sugar - likely increases the risk of CVD. At the very least, a substitution with refined carbohydrates will expand the collective waist line of a population. And this is a problem, as Denmark's strategy will almost assuredly increase the consumption of refined carbohydrates.
For the past forty years, Americans have experienced what happens when saturated fat is demonized. Industry replaces saturated fat with either trans fats (because they mimic saturated fat) or with sugar (because palatability leaves with the fat). And how do home cooks replace saturated fat? They don't simply use canola oil rather than butter. Instead, they do what's easy: eat more carbohydrates and buy foods that are nothing more than industrially produced oxymorons. Besides, the most obvious problem with today's diet is the lack of whole foods.
One of the first tenants of the food movement is to de-emphasize individual nutrients. Mark Bittman, a commentator for the New York Times, would likely agree. Yet he readily deplores saturated fat. What's more, Bittman conflates saturated fat with obesity. No one thinks saturated fat has anything to do with obesity - not the low carb crowd, or the calories counters. Public health authorities (and food policy commentators) need to get the facts straight about saturated fat, and then focus on the obvious.
The major problem facing nutrition and food is the processed carbohydrate, especially sugar. Table sugar, or sucrose, like alcohol, does not need to be consumed in any amount. It offers no nutrition and can (and likely does) only cause harm. But it is a wonderful treat and is part of our food culture - there's nothing wrong with some birthday cake - so like alcohol, it's a reasonable candidate for taxation. Saturated fat, on the other hand, comes from whole foods and is usually accompanied by important nutrients; not to mention that foods with saturated fat are delicious and also part of our food culture.
I'm not just stubborn about food taxes (see picture above), or a nihilist about food policy. I want to go after the right target. So if taxes will be employed to reduce the consumption of deleterious foods, or to generate revenue to combat the economic burden of diet-related diseases, then let's finally get over saturated fat, and start going after the obvious problem - the 32 oz. sodas that people regularly mainline.
Over the summer, I had a friend ask me how to address a common problem: he found his chicken dinners less and less inspiring. This is nothing to be ashamed of. It can happen to anyone. The best solution is to spice it up...literally.
I can relate to running out of inspiration. For those of us who restrict foods because of food-reaction, diet, or food-quality reasons, it's good to have an arsenal of flavorings ready. I've come to eating hamburger steaks very often during the week because it's a satisfying carb restricted meal, and because I can afford the grass-fed ground beef - more than steaks, anyway. So, I've been relying heavily on different spice rubs for the burgers.
Costco BBQ rubbed hamburgers.
As a general rule, I think rubs, both dry rubs and wet rubs, also called pastes, are far superior to marinades. Dry rubs taste great when you cook the meat immediately after applying the rub, but they also get better with time. Putting a dry rub on meat the night before is spectacular. Marinades, on the other hand, seem to need an unnecessary amount of time to do their work.
The most important thing, though, is that rubs consistently accomplish what they are supposed to do - impart a desired flavor. Marinades are alluring, they immediately make you think of garlic infused chicken breasts or juicy lemon-pepper fish, but they rarely come through for me. My marinades always result in bland-tasting, albeit well salted, meat that doesn't brown well due to the extra moisture. Rubs always deliver. Jerk rub will taste like a Jamaican vacation, and an herbed garlic paste will make your palate sing.
Now, that's not to say that marinades never work. They just don't work as often as I would like them to. So instead of marinading the same old chicken, here are a few of the rubs that I like to employ. Also great on pork, and some will work on beef (Jerk rub and Costo BBQ rub).
Multi-pepper rub (during last minute of grilling, brush maple syrup on meat to add a touch of sweat):
And don't forget, you can always buy rubs at the store. I like Costco's mesquite rub - smokey, spicy, and sweet. Yes, it's very strong. So it's great to use on pork and beef, or dark-meat chicken, rather than fish or white meat chicken, and it does well with a healthy dose of lime juice after cooking.
Costco Mesquite BBQ seasoning.
Hopefully my friend will recover from his chicken-woes. Although I can't help him with his first resistance to using rubs, as astute as the observation is, that raw chicken is gross to touch.
I've recently developed an obsession with 88% dark chocolate that I can find on sale at Sprouts. It has about as much fiber as it does sugar, and it's bitterness verges on espresso. I've prescribed myself to a near-nightly dose of it after dinner. And one night, while I was medicating, I came across a new study and some responses to the study that got me thinking about how easy it is to be critical about data that do not conform to our preconceived notions.
A meta-analysis was recently published on the effects of chocolate consumption and cardiovascular disease (the full text article can be found here). The analysis only included 7 studies: 6 cohort studies, one cross-sectional study, and no randomized controlled trials. Needless to say, I was surprised by the relative strength and consistency of the findings.
Source: Buitrago-Lopez et. al British Medical Journal 2011.
The various levels of chocolate intake were associated with a 37% decrease in the risk of any cardiovascular disease, and a 29% decrease in the risk of stroke. This is indicated in the figure by the diamond-shaped confidence intervals, which represent the risk of the combined studies, stratified by cardiovascular outcome, hovering around estimated relative risks. There was no association between chocolate intake and heart failure, as you can see by the respective diamond crossing the relative risk axis of 1. Unfortunately, none of these studies measured CVD mortality or total mortality, so we don't know if this reduced CVD risk was associated with a longer lifespan.
If you've been following my previous posts, then hopefully you've taken note that all of these studies are observational rather than randomized and interventional. This makes this type of data prone to confounding variables (although many of these studies corrected for numerous confounders) and bias. The bias is especially worrisome given that chocolate is somewhat of a luxury that probably associates with discerning palates, and because of all the marketing buzz regarding cocoa's abundance of antioxidants.
Even the authors are dubious of their findings since chocolate has more than just antioxidant-rich cocoa. "The high energy density of commercially available chocolate (about 500 kcal/100 g) means excessive consumption will probably induce weight gain, a risk factor for hypertension, dyslipidaemia, diabetes, and cardiometabolic disorders in general." And they didn't even mention sugar, which I'm more concerned about than calories. And others are quick to point out that the association may very well not be due to the chocolate, as I mentioned above. Marion Nestle, at FoodPolitics, concurs: "wisely, the authors point out that much more research is needed to confirm these benefits, not least because the studies were observational, not clinical trials."
I agree with all of these issues. And personally, I need substantial evidence to convince me that a food is not just food, but is actually therapeutic. But if we are going to be skeptical about chocolate because of insufficient evidence, shouldn't we be just as skeptical of other foods or nutrients with similar insufficient evidence?
My last post on meta-analyses featured a study by Siri-Tarino et al. that concluded that prospective cohort studies show no association between saturated fat intake and CVD*. Chocolate, on the other hand, does show a benefit, even in studies with similar design. Furthermore, the reduction in the risk of stroke appears greater than might be expected from abstaining from processed meat. Despite these difference, recommendations to reduce saturated fat abound, while poor chocolate only gets criticism.
Again, we have to be skeptical about all of these studies until there is either sufficint clinical trial data, overwhelming epidemiological data, or preferrably, a combination of clinical trials, epidemiology, and laboratory experiments. It's imprudent to disparage a study because chocolate "just can't be healthy" or quickly agree with an association becuase processed meats "must be bad for you." We have to be equally critical of all studies of the same methodology, regardless of the outcome.
As with coffee, I'm not convinced that chocolate is a health food or will prevent heart disease; although if you can restrain yourself, it certainly doesn't appear harmful. And with more investigation, perhaps chocolate will be definitively healthy. So until we have more conclusive evidence, eat chocolate because it is divine, because we can mull over the richness of it will friends at the dinner table, and because it is the perfect end to a meal. And be equally skeptical of claims for all foods, regardless of how sweet, sweet, delicious they may be.
*As I described in the previous post, and to be accurate, there have been clinical trials to investigate the benefit of saturated fat reduction. Replacing saturated fat with polyunsaturated fat does indeed lower the risk of cardiovascular disease. Although it does not appear to reduce CVD mortality or total mortality.
"The great tragedy of Science (is) the slaying of a beautiful hypothesis by an ugly fact"
- Thomas Henry Huxley
I eat butter. Plenty of it. And I also started rendering lard and beef tallow for cooking. Not many people my age (26) have ever seen someone render lard, let alone use it readily. The reason I use these fats is because they are delicious, and because I can buy them at the farmers market. The conventional wisdom is that I should be scared - or nearly terrified - of saturated fat. Just take a look at this YouTube video from the U.K (see below).* The eerie lighting and tone of the television announcer is enough to make me worry, but let's take a look at some recent evidence regarding saturated fat and heart disease to see if the sink analogy is apropos.
The reason that saturated fat has been demonized by the nutrition community is because it is the cornerstone of the Lipid Hypothesis. The Lipid Hypothesis, which is more of a concept than a working hypothesis, proposes that dietary saturated fat elevates cholesterol in the blood, specifically LDL cholesterol, which in turn causes atherosclerosis. Cardiovascular disease (CVD) is characterized by atherosclerosis (plaque in the arteries) and includes coronary heart disease (CHD; atherosclerosis of blood vessels in the heart) and cerebrovascular disease (atherosclerosis of blood vessels in the brain leading to stroke).
Source: Wikipedia. Myristic acid, a saturated fat
The Lipid Hypothesis has always had its critics, but it has generally been accepted as fact. However, the totality of evidence is a bit fuzzy, as many studies are contradictory or only show a small benefit from restricting saturated fat. But since CVD is the leading cause of death in the U.S., public health authorities argue that any intervention, even if it's small or somewhat uncertain, will be beneficial to the health of the population. These circumstances are ideal for what medical researchers call a "meta-analysis."
Simply put, a meta-analysis is a single study that combines the results from numerous smaller studies to form an artifical mega-study that will have enough statistical power (ability to detect a difference between the control and experimental group) to determine what the true impact of an intervention is. The goal is to walk away with an actual number, such as a relative risk or mortality statistic. For a meta-analysis to be valid, the included studies must be sufficiently similar and test the same exposure-outcome hypothesis, e.g. dietary saturated fat causes heart disease. And researchers will further restrict their inclusion criteria to well designed studies. But even with these criteria, you might ask: if I lump all these studies together, doesn't that falsely give equal credibility to both good and not-so-good studies?
Researchers address the issue of good, better, and best studies by "weighting" the different study results. This means that each study will have more or less impact on the final outcome measurement - again, such as the relative risk for heart disease - depending on the quality of the study. What makes one study better than another? Usually the size of the study (10,000 subjects is likely more accurate than 1,000), the number of confounders adjusted for (older studies might only correct for age and smoking status, whereas a newer study might have adjusted for age, smoking, socioeconomic status, cholesterol, fasting glucose, etc.), and the quality of the methods used (in a diet study, a trial that provided all of the food for the subjects is much more reliable than giving subjects a questionnaire to determine what they ate). Once you have all the studies tabulated and weighted, then you can get a summary outcome measurement and a neat graph that looks something like this:
Fig 1. Anatomy of a meta-analysis
Every meta-analysis has a graphic like this (Fig. 1), and usually they have several more depending on how many hypotheses are being investigated. The x-axis represents the relative risk. If you remember from my last post, a relative risk of 1 means no difference in risk between groups, whereas a relative risk greater than 1 indicates that the "experimental" group has more risk than the control group. Each study included in the graph is represented by a hash; the length of the hash represents the 95% confidence interval for the relative risk of that study. If you are unfamiliar with statistics, the 95% confidence interval shows the range of numbers that we are reasonably confident includes the true effect of the experiment. A smaller interval means you are more confident of the real number. All you need to know is that if the confidence interval intersects the vertical line, then our safest bet is to conclude that there is no difference between the groups, since the relative risk is likely to be 1. If the confidence interval does not intersect the vertical line, then we can conclude with reasonable certainty that there is a difference in risk between the groups. At the bottom of the graph there is a diamond that represents the confidence interval derived from all the (weighted) studies included in the meta-analysis. As you can see in the example, the diamond does not intersect the vertical line, and so the relative risk of all the studies combined is 0.85. This would mean that the totallity of the evidence, based on this meta-analysis, indicates that the treatment reduces the risk of whatever outcome by 15%.
This is virtually all that you need to know in order to interpret a meta-analysis. And if you are still reading this post, now it's time to talk about saturated fat. Several large meta-analyses have been published in the past couple of years, and they all seem to give roughly the same answer.
In 2010, Siri-Tarino et al., published a meta-analysis on prospective cohort studies that evaluated the assocation of saturated fat with cardiovascular disease. Based on 21 studies, they find no difference in the risk of CVD (the confidence interval contained 1), and conclude that "there is insufficient evidence from prospective epidemiologic studies to conclude that dietary saturated fat is associated with an increased risk of CHD, stroke, or CVD." Interestingly, they assert that there is evidence of publication bias.** But as the authors correctly point-out, this meta-analysis was limited to cohort studies and not powered enough (not large enough) to analyze the effect of replacing saturated fat with specific nutrients, such as carbohydrates or polyunsaturated fats (PUFA; think walnuts and seed oils). Fortunately, other meta-analyses have.
Mozaffarian et. al performed a meta-analysis on randomized controlled trials that replaced dietary saturated fat with PUFA. They only looked at myocardial infarction (heart attack) and CHD death; these are known as "hard endpoints," as heart attacks and death are not usually mis-diagnosed. They show that increased PUFA intake (from 5% of daily calories to 15%) in place of saturated fat reduces the combined risk of heart attack and CHD death by 19% (Fig 2). However, when the analysis isolated people who did not have pre-existing CHD, the aforementioned benefit disappeared (became statistically insignificant). And there was no benefit seen in total mortality. That is, replacing saturated fat with PUFA did reduce CHD and CHD death, but the risk of dying from all causes remained the same.
What saturated fat is replaced with is not trivial. Mozaffarian et al. also analyzed studies that replaced saturated fat with carbohydrates and monounsaturated fat (think olive oil). The single randomized controlled trial showed that replacing saturated fat with carbohydrate had no benefit, and in cohort studies, carbohydrates appear to increase the risk of CHD. Monounsaturated fat is expected to lower the risk of CHD because of its beneficial effects on the cholesterol profile, but this has not been tested in a randomized controlled trial, and pooled analysis of available cohort data show a borderline increased risk of CHD (Fig. 3). Weird, huh?
And lastly, The Cochrane Collaboration has recently published an updated meta-analysis on the effect of dietary fat reduction and/or modification (PUFA instead of saturated fat) interventions, in randomized controlled trials, on cardiovascular outcomes. Similar to their previous study and the aforementioned meta-analyses, they find that reducing and/or modifying dietary fat intake, for greater than six months, reduces the risk of CVD (events, not deaths) by 14%. This decrease is attributable to:
"studies of fat modification and reduction (not studies of fat reduction alone), seen in studies of at least two years duration, in studies of men (and not those of women), and in those with moderate or high cardiovascular risk at baseline (not general population groups)."
This means that there is a small benefit from replacing some dietary saturated fat with unsaturated fats, but this may only apply to men and those who are at risk of or already have CVD. And again, with a "high quality of evidence" given the shear number and size of the studies included, reduction of fat intake or modification of fat intake did not decrease the risk of CVD mortality or total mortality.
To be a bit critical, meta-analyses are far from perfect. Remember, they are simply a pooling of results that improves statistical power in order to weed-out a result. They do not improve the quality of the data or the individual studies themselves. An accurate colloquialism is that a meta-analysis of garbage is still garbage. Given their difficulties, I wouldn't go out and replace all of my butter with vegetable oil and expect a precisely 14% decrease in my risk of CVD. But they give a nice summary of the evidence.
In the case of saturated fat, there is consistency between these analyses. Total dietary fat is irrelevant to heart disease. Replacing saturated fat with polyunsaturated fat modestly reduces the risk of cardiovascular disease, whereas replacing saturated fat with carbohydrate has no effect and may be harmful (if it's refined carbohydrates or sugar). But at the end of the day, modifying or decreasing saturated fat likely does not decrease the risk of dying from heart disease and certainly has no effect on total mortality. So after looking over these meta-analyses and bouncing it off of my current understanding of diet and diease, here is my conclusion: there is clearly no over-whelming evidence that saturated fat is bad, and in fact, there doesn't really seem to be any evidence. And if it replaces sugar (butter instead of jam on toast), then it might actually be "healthy." And yes, I'm aware of how crazy that notion sounds. So what is one to do?
There are plenty of people who have given up butter and whole fat milk because of trepidation about saturated fat bringing them to an early grave. Or in the words of Michael Pollan from In Defense of Food, "over the last several decades, mom lost much of her authority over the dinner menu, ceding it to scientists and food marketers (p. 3)." Since the message to restrict saturated fat was loud enough to disrupt dinner, it is shocking that the evidence seems to have vanished. And this is why the conventional wisdom will not change overnight. Marion Nestle, a nutrition professor whose schtick I otherwise like, wrote a post on her blog to acknowledge these recent publications, but she inexplicably fell short of saying that saturated fat is probably harmless. So in my opinion, it seems that the facts have ruined yet another hypothesis, because clearly, butter isn't out to get you.
* Ignore the impossibility that the "saturated fat" in the video is liquid in the refrigerator but solid at room temperature in the drain. Saturated fats (coconut oil, beef tallow, butter) are solid in the refrigerator AND at room temperature.
** Smaller studies showed an increased risk of CVD from dietary saturated fat, but larger studies, which will always be published since they are well-known and anticipated, showed an equal distribution of increased, decreased, and neutral risk. The implication is that smaller studies that showed a detrimental effect of saturated fat were published, whereas smaller studies that showed no effect or a beneficial effect of saturated fat were either not submitted for publication or not accepted for publication.


























{kind=link}
{kind=link}