 |
| Source: Wikipedia. I would have had some if it looked this good... |
There’s few things more ironic than walking into a lecture titled “the molecular biology of hepatic steatosis” and being met by a table stacked with pizza and soda. Of course, the molecular biologists in the crowd weren’t the ones with non-alcoholic fatty-liver disease (or NAFLD), but it’s hard to ignore the dissonance. Fortunately, the talk was better than the lunch offerings.
The lecture was by a medical researcher who investigates the molecular mechanisms behind fatty liver disease. Today he was highlighting his group’s most recent work on the molecular mechanisms connecting obesity to liver fat deposition.
 |
| Source: Wikipedia. Adipocytes (fat cells). |
The researcher wanted to address several hypotheses. The first hypothesis is that when people become obese, their fat cells enlarge (rather than multiply) to a point that induces cellular stress. This stress then produces a cascade of intracellular signals that tell the fat cell (adipocyte) to begin apoptosis (intentional cell death). The troubled fat tissue then secretes deleterious cytokines, or hormone-like chemicals.
 |
| Source: Wikipedia. A Macrophage. |
The second hypothesis is that these cytokines recruit immune cells – specifically macrophages, an important cell of the innate immune system – that begin to engulf the fat cells. The combination of dying fat cells and macrophages causes a big problem.
When fat cells become too large, and start dying off, they dump their fat content into the circulation – like an overstuffed cream-filled donut. This results in a surplus of free fatty acids floating around the body. And this is important because two-thirds of the fat in the livers of people with NAFLD are derived from the circulation. And it isn’t just the adipocytes causing trouble.
Macrophages enjoy company, so they recruit more macrophages by secreting cytokines that have wonderful names such as Tumor Necrosis Factor alpha and Interleukin-6. These chemicals, and many others, create a vicious cycle whereby inflammation produces more inflammation produces more information. The inflammation in the fat then appears to spill out into the circulation and reach the liver.
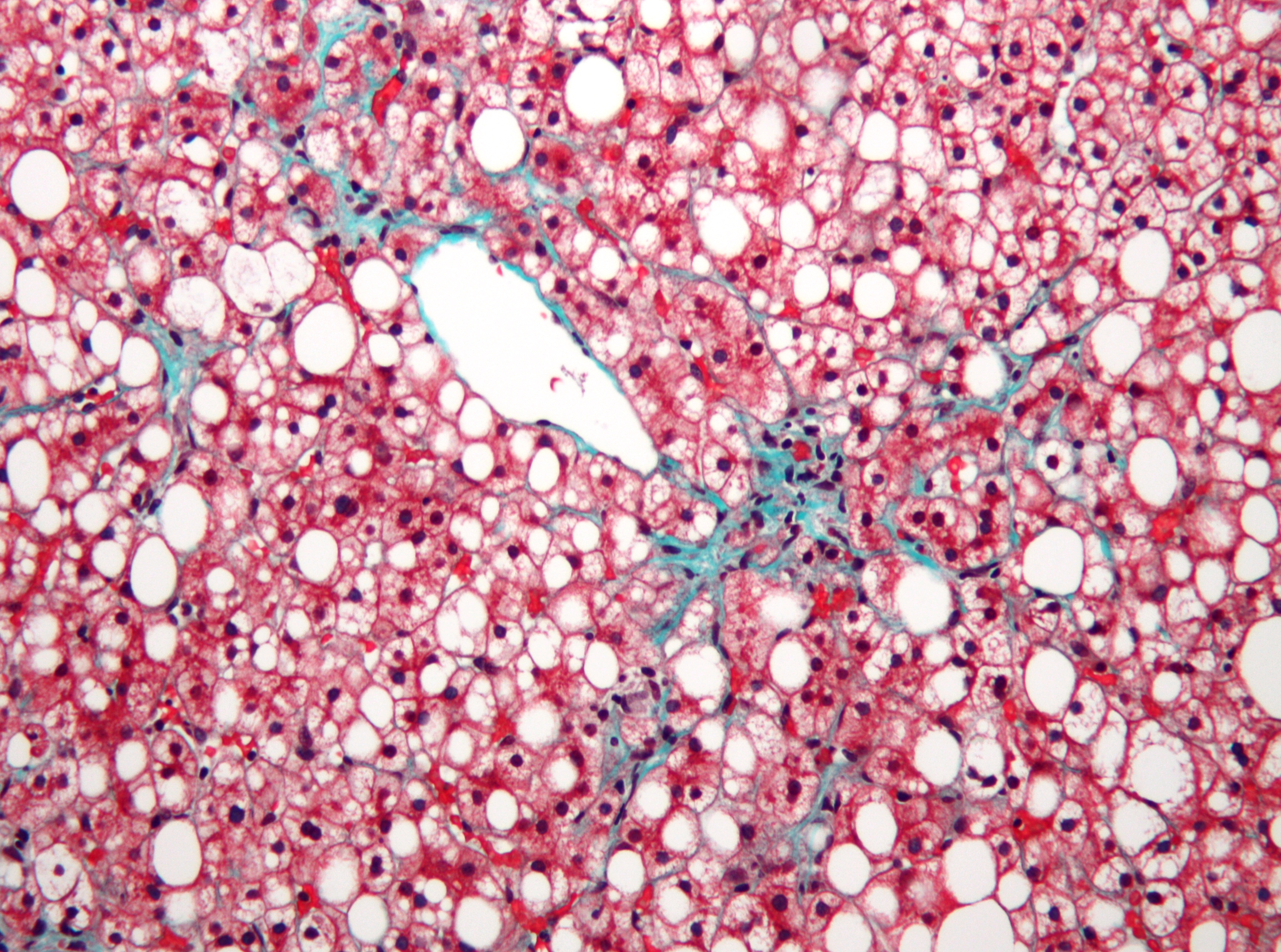 |
| Source: Wikipedia. Not-alcoholic fatty liver disease. Liver cells are pink, the white is fat that shouldn't be there... |
Inflammation in the liver leads to dysfunctional fat metabolism. The liver then begins producing too much fat, which also accumulates in the liver. The excessive free fatty acids in the circulation and the dysfunctional fat metabolism in the liver account for virtually all of the excess fat seen in NAFLD. This fat then begets more inflammation.
The excessive fat and inflammation in the liver, and the fat from inflammation, generate a lot of oxidative stress in the liver. This oxidative stress produces more inflammation, and causes the liver cells to dye off. This can lead to a clinically inflamed liver (steatosis hepatitis) and even cirrhosis (think alcoholic). At least, according to the researcher's hypothesis.
The researcher had plenty of data from cell cultures and mice, each experiment clearly showing an increase in relevant proteins and genes in response to diet-induced NAFLD. He also cited a clinical trial that showed that vitamin E (an anti-oxidant) supplementation was more beneficial than the insulin-sensitizing drug metformin in patients with confirmed NAFLD. Although, admittedly, the anti-oxidant treatment didn’t seem to be that much of a better treatment. But perhaps oxidation is indeed the culprit, and Vitamin E just isn’t a strong enough anti-oxidant.
The obesity to inflammation to fatty liver (and other problems) is a compelling hypothesis, and it has plenty of support in the research community. If this hypothesis with stands the test of time, then it would support the notion that whatever makes us fat (sugar ‘cough’ and ‘cough’ white flour), probably also leads to insulin resistance, fatty liver, and all the other diseases associated with the Western diet. But however it goes, I’m still glad that I brought tuna, broccoli, and buttered brown rice instead of chowing down on cheap pizza and soda.
From Peter...not sure why comments weren't working:
ReplyDelete"Interesting read!! Oh the whoa’s of sugar!! Have you heard any recent feedback on the impact of sugar substitutes on the diet? I’m guessing they introduce a whole new set of problems…"
Peter,
ReplyDeleteThere's definitely a lot of opinions about artificial sweeteners.
Real food advocates bemoan them on the principle that artificial sweeteners are, by definition, synthetic. And therefore, probably bad.
Most dietitians seem to want to limit them because of the precautionary principle - we don't KNOW that they cause no harm, as that is a very difficult thing to prove (or come sufficiently close to proving).
And I know there is at least one researcher who implicates them in the rise of type 2 diabetes; she proposes that they chronically elevate insulin secretion (although minor) and this eventually "wears out" the pancreas. She received the Banting Medal at the recent American Diabetes Association meeting, so she is a well respected researcher.
Personally, I'm not ready to blame them for much, especially if eaten in reasonable quantities (a few Splenda packets a day). For one, they don't contain fructose. It's the excess fructose in high-sugar diets that is especially problematic. What's more, obesity and diabetes existed before the advent of artificial sweeteners. So until there's enough evidence saying otherwise, I'm going to stick with Ockham's razor and maintain that table sugar is the primarily problem. Although it could be both...we'll just have to see.